Irregularly Irregular
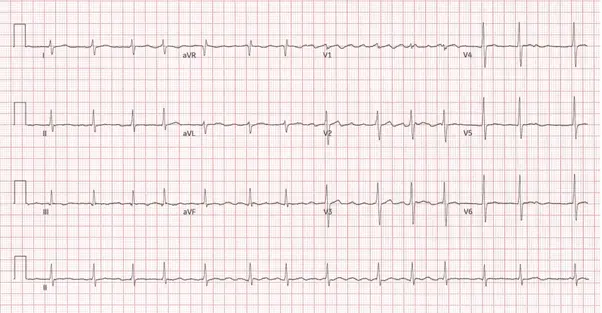
What AFib Looks Like on an ECG
No visible P waves — a chaotic, wavering baseline replaces the normal flat line between beats, and QRS complexes fall at unpredictable intervals. This “irregularly irregular” pattern is the hallmark of AFib and can be confirmed with a simple 12-lead ECG in the clinic.